Nearterm Blog
Revenue Cycle Management In 1951: It Used to be a Lot Easier…Or Was It?
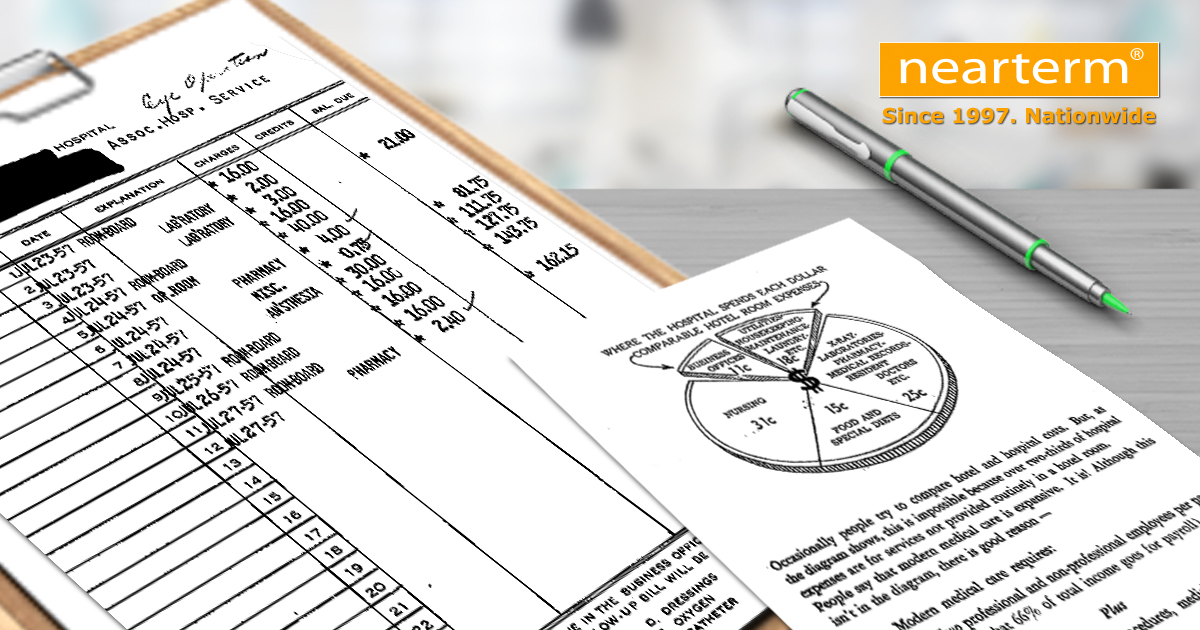
The above image is an actual hospital bill and accompanying explanation of charges used in 1951. Just think of the things that we didn’t have to manage back then. A short list might include coding, claim edits, massive denials, contract payment compliance, Medicare/Medicaid (both started in 1965), managed care contracts, HIPPA regulations, “patient-friendly” billing initiatives, use of technology, and outsource considerations.
We now embrace in stride all of the complexities that have evolved since this bill was produced. In fact, increasing complexity is the “new normal” in our business. The explanation of charges that accompanied this bill was actually pretty transparent for the time and was largely designed to help patients understand the difference between hospital and hotel costs. It was easy to understand the bill and the explanation. However, the expressed complexities that have emerged today make itemized bills almost unintelligible and our explanations often lead to more skepticism than acceptance. It’s not easy anymore!
In our company and in your hospital, we are attuned to customer service management and its importance in the revenue cycle continuum. Among revenue cycle and financial professionals, part of our jobs back in 1951 and presently today has always included the mantra “cash is king.” But today, more than ever, patients are decision makers. I can remember a time early in my career when my boss imparted to me that our “internal client” or “customer” was the physician because it was the physician who drove patients and therefore revenue to our facility. Now we have several customers, which is yet another added complexity.
However, in the shadow of all the differences one can enumerate between 1951 and today, there is one glaring similarity. Healthcare revenue cycle management success is still about blocking and tackling. It still means the presence of a compassionate patient access process that results in a positive patient experience, while simultaneously recording data that enables us to populate a clean claim and collect revenue. It still means timely, accurate revenue capture and billing. It still means effective follow-up on billed AR and prompt recognition of collectability. Like you, our consultants, interim leaders, and staff augmentation specialists at Nearterm realize the importance of keeping our eyes on the prize – CASH IS STILL KING.
Oh well, maybe things haven’t changed after all! ?
Jim Matthews
Principal, Nearterm Corporation
